Maybe you’ve seen folks on the interwebz going sort of crazy over B12 deficiency and folate deficiency, saying that they have the MTHFR issue, hypochlorhydria, or all sorts of other reasons why they simply can’t get enough B12 and/or folate from foods alone.
I say that they’re probably wrong on the true root cause of their problem, and they are overlooking something that is pretty well-established in the research to cause Vitamin B12 and folate deficiency…and that is the POISON called “Vitamin A” depleting it out of their bodies, all day, every day.
First, is there an epidemic of Vitamin A toxicity going on currently? Yes, see my video here for that evidence.
Next, the studies that I’m going to post below are about the form of Vitamin A known as 13-cis retinoic acid, which is created/converted by the body from the Vitamin A (carotenoids or retinoids) that you consume. See below. Remember that endogenous means “originating within the body”.
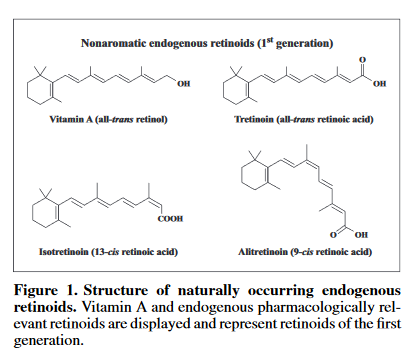
Image above taken from paper Retinoid treatment of skin diseases.
Pay attention to the following terms in that image:
- Endogenous – originating within the body
- Isotretinoin (13-cis retinoic acid)
- Naturally occurring
- Pharmacologically relevant
This is all extremely pertinent to what I’m about to talk about. When 13-cis retinoic acid is in the body, it is said to be “endogenous” and “biologically active”. However, when people take a pill of 13-cis retinoic acid, it’s called ACCUTANE or ROACCUTANE. Did you know this?
Did you know that your body takes Vitamin A you eat and makes it into the same compounds as those known EXTREMELY TOXIC DRUGS? If no one else is going to tell you, let me be the first. If you’d like to see even more evidence that this is true, along with how natural forms of Vitamin A are just as toxic as synthetic forms of Vitamin A, see my video here for that information (with full references).
So, now that we have established that the 13-cis retinoic acid that your body makes from Vitamin A that you eat is exactly the same as the 13-cis retinoic acid that people take in pharmaceutical pills (please don’t argue they are different any longer without any evidence to back your statement up), then we can logically link the side effects of 13-cis retinoic acid aka isotretinoin aka Accutane aka Roaccutane with Vitamin A intake.
If a person is taking in Vitamin A (including carotenoids like beta-carotene that end up going down the exact same pathways), then they are creating 13-cis retinoic acid in their body, and it will do all the nasty things that this compound is known for (see here for a list of isotretinoin side effects).
Let’s do some association. If you believe Vitamin A is an essential vitamin, and the science says that you turn Vitamin A into the Accutane molecule in your body as one of the “active” forms of Vitamin A…how, therefore, can the ACCUTANE MOLECULE be both so TOXIC and yet ESSENTIAL at the same time? The simple answer is that it CANNOT BE BOTH. This really needs to sink in, people!
On to the Vitamin A-induced B12 and folate deficiency papers. I don’t need to comment on these, they really do speak for themselves, and there are a lot of them. If you get to the very last one, there are some fun surprises at the end:
Decreased Vitamin B12 and Folic Acid Concentrations in Acne Patients After Isotretinoin Therapy: A Controlled Study
“In total, 120 patients with moderate and severe acne vulgaris who completed 6 months isotretinoin therapy and 100 healthy individuals who constituted the control group were included in the study. […] A statistically significant decrease was detected in post-treatment vitamin B12 and folic acid levels.”
Effect of isotretinoin treatment on plasma holotranscobalamin, vitamin B12, folic acid, and homocysteine levels: non-controlled study
“Some previous studies reported elevated homocysteine (Hcy) levels after treatment with Iso. Some side effects have clinical presentations similar to vitamin B12, folic acid deficiencies, and hyperhomocysteinemia. In the present study we evaluated the plasma Hcy levels, the vitamins involved in its metabolism (vitamin B12 and folic acid), and holotranscobalamin (HoloTC), a transport system for vitamin B12 absorption in patients receiving Iso treatment for acne vulgaris. […] Posttreatment vitamin B12, folic acid, and HoloTC levels were significantly lower while Hcy levels were significantly higher compared with initial values.”
Homocysteine, folic acid, and vitamin B12 levels in patients on isotretinoin therapy for acne vulgaris: A meta-analysis
“Results: A total of 10 studies consisting of 592 patients were included in the meta-analysis. Plasma Hcy levels were significantly increased after Iso therapy, whereas folic acid levels were significantly decreased after Iso therapy.”
Efficacy of Folic Acid and Vitamin B 12 Replacement Therapies in the Reduction of Adverse Effects of Isotretinoin: A Randomized Controlled Trial
“We conducted a randomized controlled trial to investigate whether folate and vitamin B12 replacement therapy with isotretinoin would be useful for preventing hyperhomocysteinemia. A total of 66 patients with acne were randomized into two groups: group A took isotretinoin, folic acid, and vitamin B12, whereas group B took isotretinoin alone. Treatment was continued for 2 months. Blood homocysteine, folic acid, and vitamin B12 levels were measured before and after treatment. In group A, a significant decrease in homocysteine level was observed after treatment (P=.0004), although it was still within the normal range. Folic acid and vitamin B12 levels significantly increased. In group B, no significant changes were observed in the levels of homocysteine and vitamin B12, but folic acid levels decreased significantly.”
Successful Treatment of Isotretinoin Induced Musculoskeletal Pain by Vitamin B12 and Folic Acid
“We reported six patients with nodulocystic acne who reported musculoskeletal pain after taking isotretinoin which successfully treated with daily supplementation of folic acid and B12.”
Severe aphthous stomatitis secondary to vitamin B12 deficiency with isotretinoin therapy
“The progressive development of glossitis and oral ulcers during the second cycle of isotretinoin therapy, together with the absence of evidence suggestive of pernicious anemia or inflammatory bowel disease and the lack of recurrence after treatment discontinuation, strongly suggest that the development of vitamin B12/folate deficiency in our patient was strictly related to isotretinoin therapy.”
Vitamin B12 and folate deficiency anaemia associated with isotretinoin treatment for acne.
Oral isotretinoin is reserved for severe acne because of the potential side‐effects. We report a case of anaemia due to B12 and folate deficiency developing 8 weeks after treatment with isotretinoin for acne.
[…]
On the eighth week of treatment, she started to feel tired and dizzy. One week later, she felt sick, with epigastric pain, vomiting and diarrhoea. On admission to hospital she looked pale, with a pulse rate of 90 beats/min and normal blood pressure and temperature. She had extensive crusting around the mouth with erosions of the lips and redness of the buccal mucosa. She also had multiple painful perianal ulceration.
[…]
The patient’s isotretinoin was discontinued on admission to hospital and she was treated with B12 and folate supplements with rapid improvement, correction of her anaemia and normalization of her white cell count. She was discharged in good condition and remains well.
[…]We report an interesting association between B12 and folate deficiency anaemia with isotretinoin treatment for acne. Our patient was clinically well before isotretinoin treatment, and her symptoms stopped rapidly after discontinuation of isotretinoin and initiation of B12 and folate replacement. The mechanism of her B12 and folate deficiency is not entirely clear. In this case, anaemia and neutropenia occurred possibly because of B12/folate deficiency or direct drug toxicity. More likely, an accelerated development of isotretinoin toxicity (with colitis) resulting in B12/folate deficiency anaemia in a marginally deficient but clinically normal patient led to the development of the symptoms.
Depression, isotretinoin, and folic acid: A practical review
“Isotretinoin (ISO) is a first-generation retinoid discovered in 1952 and approved by the FDA for the treatment of nodulocystic acne in 1982. […] ISO can create psychiatric problems, including depression and suicidal ideation. These neuropsychiatric problems are very similar to disorders secondary to hyperhomocysteinemia (HHcy), vitamin B12, and folic acid (vitamin B9) deficiencies.”
The effects of isotretinoin therapy on serum homocysteine, folate and vitamin B12 levels in patients with acne: a metaanalysis and meta-regression
“Studies have revealed changes in the serum level of homocysteine, folate and vitamin B12 in patients with acne receiving isotretinoin treatment; however, the results were inconsistent.2,3 Hyperhomocysteinemia and deficiency of folate and vitamin B12 following isotretinoin therapy may potentially increase cardiovascular and neuropsychiatric risks.4,5 We sought to examine this potential side-effects by conducting a meta-analysis and meta-regression.
[…]
Twelve studies involving 684 patients were included. The characteristics of the included studies were summarized in Table 1. After isotretinoin therapy, homocysteine levels significantly increased, folate levels significantly decreased, and vitamin B12 levels remained unchanged. Subgroup analyses revealed similar results after isotretinoin treatment for 1–2 and 3–4 months. A meta-regression analysis revealed an association of higher cumulative isotretinoin dose with a larger decrease in folate levels. No publication bias was detected.
Mechanism of isotretinoin’s effect on the one carbon metabolism pathway was first hypothesized by Schulpis et al.6 to be an inhibitory effect on the cystathionine-b-synthetase in the transsulfuration pathway. Another hypothesis is that isotretinoin likely inhibits the remethylation pathway via folate and vitamin B12 reduction since remethylation requires 5-methyltetrahydrofolate (a folate derivative) as a substrate and vitamin B12 as a coenzyme. This prevents homocysteine from converting to methionine.
The mechanism of how isotretinoin could lead to lower folate or vitamin B12 levels is unknown. Decreased absorption of these vitamins has been suggested as a possible cause.7 Additionally, we cannot exclude the possibility that isotretinoin may cause subclinical liver dysregulation to affect folate and vitamin B12 metabolism.6
Kim et al.8 also revealed hyperhomocysteinemia and folate deficiency after isotretinoin treatment. However, they did not examine the dose–response relationship between cumulative isotretinoin dose and changes in these parameters. Based on our meta-analysis, a cumulative isotretinoin dose of 20 mg/kg would be associated with a small effect size of a SMD of -0.20 in folate levels. When the cumulative dose reaches 70 mg/kg, this SMD decreases to -0.70, indicating high sensitivity of folate level to cumulative isotretinoin dose.
[…]
In conclusion, isotretinoin may cause hyperhomocysteinemia and folate deficiency in acne patients. We also found a dose-dependent relationship between cumulative isotretinoin dose and decreased folate level.
If you’ve still been reading this far, make sure to note in that final paper that it is theorized that 13-cis retinoic acid may theoretically be negatively affecting the body’s SULFUR metabolism and/or the body’s METHYLATION processes.
All of these “modern problems” are connected. We only needed to find the connector, and we now have it. Vitamin A is only a POISON.